
Inadequate support: The claim didn’t present any supporting evidence of the alleged harmlessness of cholesterol and danger of statins.
FULL CLAIM: “Nobody has ever died from high cholesterol”; “people die from the statin drugs that they give you for high cholesterol”
REVIEW
Cholesterol and statin misinformation is widespread and can have life-threatening consequences for patients. Science Feedback previously debunked some of these inaccurate claims.
A Facebook reel posted in October 2024 claimed that “nobody has ever died from high cholesterol”. In addition, the reel claimed that people with high cholesterol actually die from the cholesterol-lowering drugs statins.
This reel is an excerpt from an interview with herbalist Alexander Hickman, who also goes by the name Yahki Rapha Elohim, on the YouTube channel Sway’s Universe in March 2024. The YouTube video was viewed more than 400,000 times at the time of writing. Science Feedback previously reviewed a misleading claim by Hickman that chemotherapy causes cancer.
Hickman’s claim about cholesterol and statins is inaccurate and directly contradicted by medical evidence, as we explain below.
What is cholesterol?
Cholesterol is a type of fatty substance that plays several important roles in our body. It’s part of the lipid membranes that form the outer layer of our cells. Cholesterol is also the raw material that produces crucial molecules like vitamin D and hormones such as estrogen and testosterone.
Most of our cholesterol—80%, in fact—is produced in our liver, and the rest comes from the food we eat. Animal fat found in red meat, dairy products, and eggs are the main sources of dietary cholesterol.
Fatty molecules like cholesterol aren’t soluble in water-based liquids like blood. To transport it, the body combines cholesterol with lipoproteins, which act as carriers. Two key lipoproteins are low-density lipoprotein (LDL) and high-density lipoprotein (HDL).
When bound to cholesterol, the LDL is referred to as LDL-C. It’s often called “bad cholesterol” because LDL-C contributes to atherosclerosis (see below). By contrast, HDL is responsible for bringing cholesterol to the liver to be eliminated, and thus reducing the risk of atherosclerosis. For that reason, it is sometimes called “good cholesterol”.
For an adult, a healthy level of blood cholesterol is between 125 and 200 milligrams per deciliter of blood (mg/dL), or 3.2 millimole per liter (mmol/L) for total cholesterol, below 100 mg/dL (2.6 mmol/L) for LDL-C, and above 40 to 50 mg/dL (1 to 1.3mmol/L) for HDL-C.
High blood cholesterol increases the risk of death
Contrary to the claim, high blood cholesterol is responsible for many deaths each year. According to the 2019 Global Burden of Disease report, 4.4 million deaths worldwide were attributable to high blood LDL-C, which represented 93 million years of life lost[1]. In 2021, the number of deaths attributed to high cholesterol was 3.7 million (Figure 1).
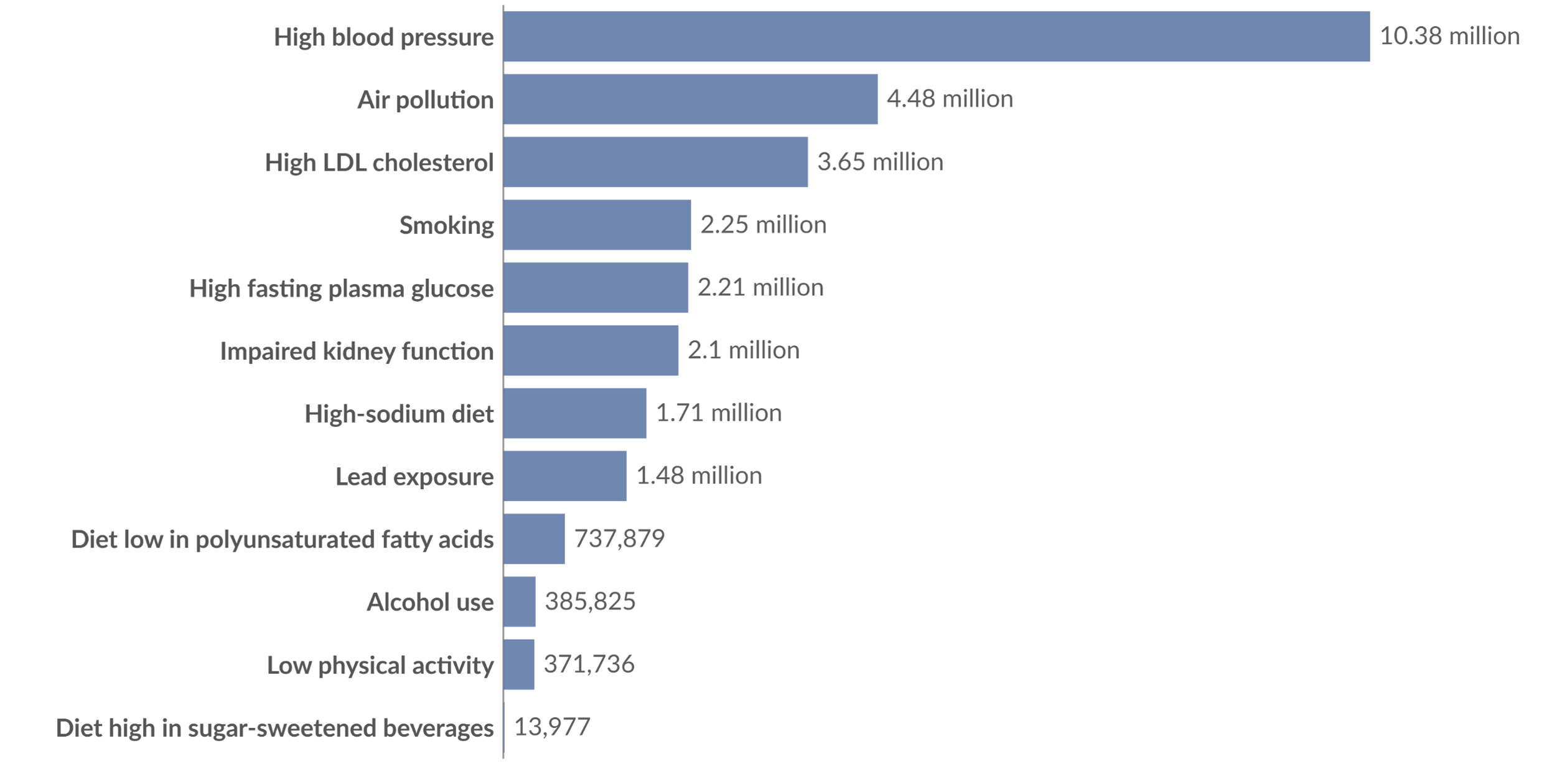 Figure 1 – Number of deaths from cardiovascular diseases by risk factor in 2021. Source: Our World in Data.
Figure 1 – Number of deaths from cardiovascular diseases by risk factor in 2021. Source: Our World in Data.
In fact, high blood cholesterol is the third-biggest modifiable risk factor for cardiovascular death after hypertension and dietary risks[1]. High blood cholesterol is dangerous because it raises the risk of life-threatening cardiovascular events, such as heart attack and stroke. This is because high LDL-C levels lead to the accumulation of LDL-C on the walls of blood vessels, forming fatty plaques called atheromas. This process is known as atherosclerosis (Figure 2).
As these cholesterol-filled plaques grow, they gradually narrow the arteries, reducing blood flow. Consequently, the tissues and organs downstream of the blockage are deprived of adequate blood supply, impairing their function.
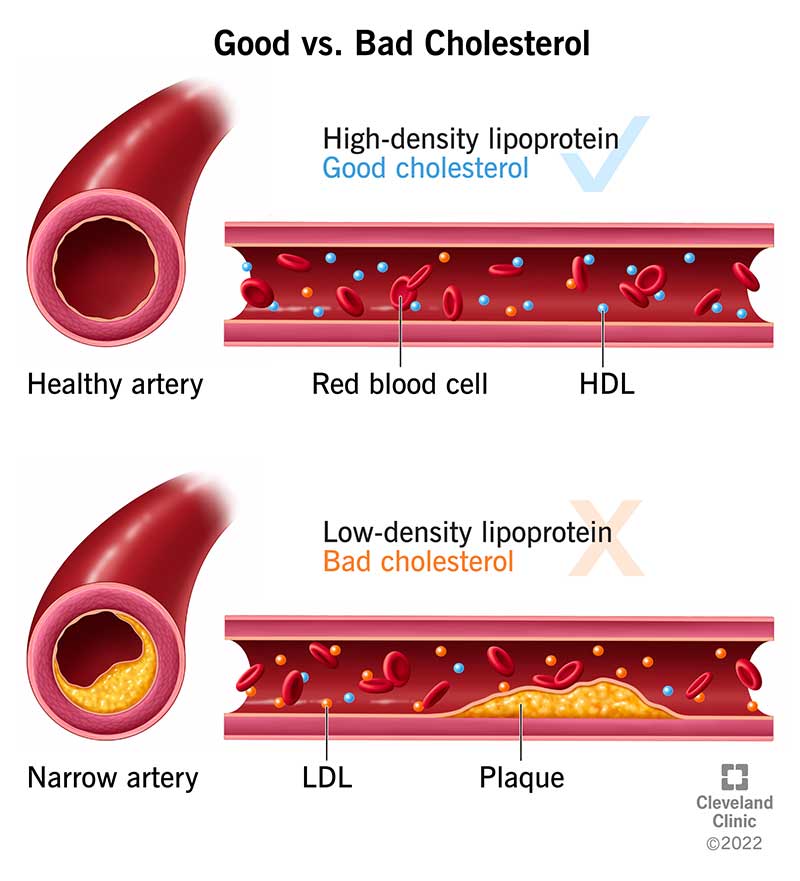
Figure 2 – The process of plaque buildup during atherosclerosis. The plaque is composed of LDL-C, cells, calcium and diverse proteins. As the plaque grows, the available space where the blood can flow decreases. When the plaque ruptures, it causes blood clotting. Source: Cleveland Clinic.
When a coronary artery—an artery feeding the heart—is clogged, it results in coronary heart disease (CHD), characterized by chest pain and shortness of breath. However, those symptoms usually appear at an advanced stage of CHD. Thus, the disease may develop undetected for years. When the blood flow is significantly reduced, it can lead to heart failure and sudden cardiac arrest.
As we can see, the obstruction of blood flow can become life-threatening over time. But the more acute danger lies in plaque rupture. Substances trapped in the plaque are released upon plaque rupture and some of these substances promote blood clot formation[2].
A blood clot may completely interrupt blood flow and deprive the tissues of oxygen. When the blood clot forms in coronary arteries, it causes a heart attack. When it occurs in brain arteries, it causes an ischemic stroke. Both can be fatal if not treated immediately.
Population-level studies and clinical trials have shown that high cholesterol increases the risk of life-threatening cardiovascular events.
In 2010, a meta-analysis evaluated the safety and efficacy of cholesterol-reducing therapies in 21 clinical trials including a total of 129,526 participants with a median follow-up of about 5 years. The results showed that lowering blood level of LDL-C decreased the risk of major cardiovascular events such as death from heart attack, non-fatal infarction, and strokes. In particular, reducing LDL-C blood concentration by 38 mg/dL (1 mmol/L) decreased all-cause mortality by 10%, and mortality due to cardiac event by 14%[3].
Another meta-analysis published in JAMA in 2016 analyzed data from 49 clinical trials of cholesterol-reducing therapies. It included more than 300,000 participants who were followed for a median of roughly four years. It found that reducing LDL-C in the blood by 38 mg/dL (1mmol/L) reduced the risk of major cardiac events by 23% and the risk of cardiovascular death and myocardial infarction by 1.5 to 4.6%[4].
Consistent with those studies, a more recent meta-analysis of 28 clinical trials following more than 186,000 participants over approximately five years years found that reducing LDL-C blood levels by 38 mg/dL (1 mmol/L) with cholesterol-lowering therapies reduced the risk of major cardiac events by 21% and the risk of cardiovascular death by 12%. Of note, the analysis revealed that the beneficial effect of reducing the blood level of cholesterol decreased with age[5].
A pooled analysis of 22 trials for the US Preventive Services Task Force found that cholesterol reduction by statin therapy was associated with a lower risk of all-cause mortality. The analysis didn’t show an effect on cardiovascular mortality but the authors noted that this was due to a trial having recruited older than usual patients and another trial with “methodological limitations”[6].
Prospective cohort studies studying the correlation between blood level of cholesterol and mortality are also available. The number of people included in these studies ranged from tens of thousands to several millions, and the follow-up duration exceeded twenty years in some studies.
Overall, these studies also pointed to the fact that mortality is higher among individuals with high blood cholesterol, confirming the results from clinical trials[7-10].
It should be noted that several studies found that a low level of LDL-C was associated with higher mortality[8-11]. However, there is no clear explanation as to the reason why. Some researchers suggested that low cholesterol could be detrimental to health[11]. On the other hand, others suggested that it could be a bias, where a very low concentration of cholesterol in the blood could be a consequence of other serious health issues[10].
Whether very low cholesterol levels are beneficial or harmful might still be open for debate. However, the one thing that both observational studies and clinical trials clearly show is that high levels of blood cholesterol, especially LDL-C, increase the risk of death. By contrast, maintaining healthy blood cholesterol levels as defined in official guidelines reduces a person’s risk of experiencing life-threatening cardiovascular events.
Statins are safe and effective at reducing cholesterol levels and risk of cardiovascular conditions
The claim that people die because of statins is unfounded.
Statins are the main class of cholesterol-lowering drugs used nowadays. They work by inhibiting a key enzyme responsible for cholesterol production in the liver. This reduces the amount of cholesterol and circulating LDL-C in the blood[12].
Furthermore, statins also protect against cardiovascular mortality by stabilizing plaques and reducing their risk of rupturing and forming blood clots[13].
Clinical trials showed that statins are effective in protecting from cardiovascular events and are well tolerated[12,14].
Like any drug, statins also come with some side effects, the most common being muscle pain. However, the use of statins isn’t associated with an increased risk of dying.
Some data indicate that statins can increase the risk of developing type II diabetes, which can be life-threatening in the long run if untreated. However this is a rare side effect that occurs primarily among patients who were already in a prediabetic state. Prediabetes is having a blood sugar level that’s higher than normal, but lower than the level seen in diabetes. That said, people with diabetes are at a higher risk of cardiovascular issues. So the small risk of statins increasing blood sugar is outweighed by their protective effect against cardiovascular events.
According to the Mayo Clinic, statins may be associated with very rare cases of life-threatening muscle damage called rhabdomyolysis when used in combination with certain drugs. However, this occurs in only a few cases per million people using statins. Given the well-proven effect of statins in reducing the level of cholesterol and improving cardiovascular health, the benefits of statins largely outweigh those risks.
Furthermore, there are now effective alternatives to statins, like ezetimibe and PCSK9 inhibitors, meaning that one doesn’t only need to depend on statins to initiate a cholesterol-reducing therapy.
Conclusion
Hickman’s claim that no one has ever died from high cholesterol is false. In fact, cholesterol is the third-biggest modifiable risk factor of cardiovascular mortality. Too much cholesterol is directly associated with atherosclerosis and life-threatening cardiovascular events such as heart attacks and strokes.
By contrast, statins are generally safe and effectively reduce the amount of LDL-C circulating in the blood. Clinical trials showed that reducing cholesterol levels with statin therapies reduced the risk of dying from cardiovascular complications.
REFERENCES
- 1 – Roth et al. (2020) Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019. Journal of the American College of Cardiology.
- 2 – Bentzon et al. (2014) Mechanisms of Plaque Formation and Rupture. Circulation Research.
- 3 – Baigent et al. (2010) Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170 000 participants in 26 randomised trials. The Lancet.
- 4 – Silverman et al. (2016) Association Between Lowering LDL-C and Cardiovascular Risk Reduction Among Different Therapeutic Interventions. Journal of the American Medical Association.
- 5 – Armitage et al. (2019) Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomised controlled trials. The Lancet.
- 6 – Chou et al. (2022) Statin Use for the Primary Prevention of Cardiovascular Disease in Adults. Journal of the American Medical Association.
- 7 – Abdullah et al. (2018) Long-Term Association of Low-Density Lipoprotein Cholesterol With Cardiovascular Mortality in Individuals at Low 10-Year Risk of Atherosclerotic Cardiovascular Disease. Circulation.
- 8 – Rong et al. (2022) Association of Low‐Density Lipoprotein Cholesterol Levels with More than 20‐Year Risk of Cardiovascular and All‐Cause Mortality in the General Population. Journal of the American Heart Association.
- 9 – Yi et al. (2019) Total cholesterol and all-cause mortality by sex and age: a prospective cohort study among 12.8 million adults. Scientific reports.
- 10 – Chen et al. (2024) Low-Density Lipoprotein Cholesterol, Cardiovascular Disease Risk, and Mortality in China. JAMA Network Open.
- 11 – Liu et al. (2021) Association between low density lipoprotein cholesterol and all-cause mortality: results from the NHANES 1999–2014. Scientific reports.
- 12 – Ward et al. (2019) Statin Toxicity: Mechanistic Insights and Clinical Implications. Circulation Research.
- 13 – Puri et al. (2015) Impact of statins on serial coronary calcification during atheroma progression and regression. Journal of the American College of Cardiology.
- 14 – Maron et al. (2000) Current Perspectives on Statins. Circulation.
