

Misleading: Numerous studies have shown that the benefits of COVID-19 vaccines outweigh their risks. It is COVID-19 that is associated with a greater risk of heart problems, blood clotting disorders, and other complications.
FULL CLAIM: “Contrary to governmental claims of mildness, the study found that most of those who reported myocarditis required emergency medical care or hospitalization, and 92 individuals reportedly succumbed to the apparently vaccine-induced affliction”; “the vaccines never stopped transmission”; “COVID-19 vaccination may pose more harm to children than theoretical benefit [...] Sweden, Norway, and Finland in 2021 [...] suspended the use of Moderna injections in young people due to the detection of safety signals for an increased risk of myocarditis”
REVIEW
An article published by the website The Blaze in late January 2024 claimed that a study published in the journal Therapeutic Advances in Drug Safety showed the risk of COVID-19 vaccination outweighed its benefits.
It cited the study’s conclusion stating that “COVID-19 vaccination is strongly associated with a serious adverse safety signal of myocarditis, particularly in children and young adults resulting in hospitalization and death”.
Similar claims also appeared in the Washington Times and on X (formerly Twitter). Overall, they received more than 6,800 engagements on social media platforms, including Facebook and X/Twitter.
As we will explain below, the article repeats a host of already-refuted claims and inaccurately portrays the risk of myocarditis posed by COVID-19 vaccination. The study that it relies on also contains important limitations and doesn’t provide reliable evidence for its claims.
VAERS reports are useful in signaling potential concerns for further investigation, but on their own cannot prove a causal link
The study in Therapeutic Advances in Drug Safety was authored by computational biologist Jessica Rose, masters student Nicolas Hulscher, and cardiologist Peter McCullough.
Both Rose and McCullough have previously spread vaccine misinformation. Hulscher, according to his LinkedIn profile, is a masters student in epidemiology at the University of Michigan Ann Arbor. Notably, Hulscher and McCullough co-authored a preprint that claimed 76% of deaths in vaccinated people were due to COVID-19 vaccines. Health Feedback covered the preprint’s questionable methods and conclusions here.
The stated aim of the study was to determine “possible links between COVID-19 vaccination and myocarditis”, using reports in the U.S. Vaccine Adverse Event Reporting System (VAERS), particularly associations between age, gender, and dose of vaccine.
It’s worth noting that the link between myocarditis and COVID-19 mRNA vaccines was already identified by studies published in 2021. These studies showed that it is young males, particularly adolescents and young adults typically below the age of 30, who are most likely to develop myocarditis, and that myocarditis is most likely to occur after the second dose[1-3].
And myocarditis has since been acknowledged by public health agencies in Europe, the U.S., Australia, and elsewhere, as a potential side effect of COVID-19 mRNA vaccination, particularly in young males.
Rose et al. reported the same trends observed in earlier studies, demonstrated by the following three statements:
“This side effect was mostly reported in young individuals, especially males.”
“Myocarditis was more likely following a second dose of vaccine.”
“individuals under the age of 30 were more prone to acquire myocarditis from COVID-19 vaccination compared to those aged 30 and above”
It also reported that there were a total of 3,078 reports, or 0.3% of all adverse events, related to myocarditis.
One of the red flags in the study shows up in the authors’ classification of these events as “COVID-19 vaccine-related”, despite the fact that VAERS reports alone are insufficient to establish that a case of myocarditis was caused by the vaccine. The same red flag appears in the authors’ claim that deaths reported to VAERS were also caused by the COVID-19 vaccines.
This is not to say that VAERS reports have no place in determining whether an adverse event could be caused by a vaccine. In fact, VAERS reports were among the data that clued the CDC into the association between myocarditis and COVID-19 mRNA vaccines. But this was only accomplished after additional investigation into the reported cases and statistical analyses.
The authors also postulated that myocarditis cases “could present as sudden death”—the language echoing the “died suddenly” dog whistle used by opponents of COVID-19 vaccination.
To do this, they cited two VAERS reports. One was a 33-year-old male whose death was attributed to myocarditis following an autopsy, and who received his last vaccine dose nearly two years ago.
The other was a 15-year-old male who became “significantly ill” four days before he died—rendering the authors’ interpretation of this as a “sudden death” debatable—and whose cause of death was attributed to myocarditis of unknown cause. According to the VAERS report, he received his last vaccine dose roughly a year ago.
However, neither of the cases above are consistent with the pattern of vaccine-induced myocarditis. Studies have observed that the onset of myocarditis symptoms typically begin within the first week after vaccination[2,4], although a range of up to a month has also been observed[5]. The U.S. Centers for Disease Control states that myocarditis due to COVID-19 vaccination most frequently occurs within seven days of vaccination.
Given the very long period of time that had passed since their last vaccine dose and the fact that myocarditis can be caused by multiple things, not just COVID-19 vaccines, the authors seem to have jumped to conclusions in attributing both deaths to COVID-19 vaccination without additional information.
Rose et al. also alleged that myocarditis after vaccination entailed a serious risk of hospitalization and death, based on their finding that “76% of cases resulted in emergency care and hospitalization”.
However, this fails to acknowledge that reporting serious adverse events after COVID-19 vaccination, regardless of whether the vaccine caused the adverse event, is mandatory. Per the VAERS website, serious adverse events include “Inpatient hospitalization or prolongation of existing hospitalization” and death.
The potential skew in reports brought about by this policy, however, wasn’t accounted for by the authors.
Contrary to the conclusions of Rose et al., several studies that examined the severity of vaccine-induced myocarditis have found that the majority of patients fully recover without any complications[4,6,7].
Finally, the authors misrepresented one of the studies it cited to support its claims, specifically a study by Swank et al. as finding “circulating Spike protein among the vaccinated with post-acute sequelae for up to 1 year”.
We reached out to the study’s corresponding author, David Walt, a professor of pathology at Brigham and Women’s Hospital and a core faculty member at Harvard’s Wyss Institute. In an email, Walt stated that this incorrectly described the study’s findings.
“It is NOT the full spike protein [detected in vaccinated people],” he said. “We found that the S1 fragment of the spike protein is detectable for three to seven days post-vaccination and is undetectable after that.”
He clarified that it was in long COVID patients that the spike protein was detected. “This is NOT caused by vaccination, but by infection,” he said.
He stated that “vaccine-induced myocarditis is very rare” and that “the levels of these proteins (S1 and spike) we are detecting in all our studies are very low. Our test is ultrasensitive. The levels are not at the concentration that would cause systemic inflammation”.
“The claims in the article are exaggerations,” he said.
Repetition of false and misleading claims about COVID-19 vaccines
The claim in the Blaze article that “the vaccines never stopped transmission” is a refrain that is echoed time and time again by those who oppose COVID-19 vaccination. As Health Feedback explained previously, the claim is an example of the “nirvana fallacy”, in which a solution is rejected simply because it doesn’t work perfectly.
Such an expectation is unrealistic as no vaccine exists that works 100% of the time.
Multiple studies have shown that the COVID-19 vaccines reduce the likelihood of an infected person transmitting the virus to others, such as between people living in the same household[8-13]. The vaccines did so with varying degrees of effectiveness, depending on factors like the variant and the amount of time that had elapsed since the last vaccine dose. Although imperfect, they did reduce transmission.
Secondly, while Sweden, Norway, and Finland did suspend the use of the Moderna COVID-19 vaccine for young men, this can in no way be interpreted to mean “Europeans […] have spared their children from the novel vaccines”. For one, Sweden, Norway, and Finland don’t restrict the use of other COVID-19 vaccines, such as the Pfizer-BioNTech COVID-19 mRNA vaccine. And many other European countries have placed no age restrictions on COVID-19 vaccination in the first place.
The benefits of COVID-19 vaccination outweigh its risks, not the other way around
The Blaze article relied on the study by Rose et al. to suggest that the risks of the COVID-19 vaccines are greater than its benefits. However, as the study didn’t undertake any examination of the benefits of COVID-19 vaccination nor did it make a risk-benefit assessment, it is unequipped to support the suggestion made by The Blaze.
Firstly, studies have shown that people vaccinated against COVID-19 are less likely to develop severe disease, to require hospitalization, and die compared to unvaccinated people[14-16]. Thus, getting vaccinated reduces the risk of COVID-19 complications, which is the primary goal of vaccination.
Secondly, while COVID-19 vaccines are associated with a slightly elevated risk of myocarditis and a particular blood clotting disorder, studies have found that the risk of heart complications, including myocarditis, associated with COVID-19 is greater than that of COVID-19 vaccines[17,18].
Indeed, the incidence of post-vaccine myocarditis has been estimated to be as high as 35.9 per 100,000 people. In contrast, that of post-COVID-19 myocarditis is 64.9 per 100,000 people[19].
The American Heart Association considers the benefits of the COVID-19 vaccines to outweigh their risks. An expert consensus by the American College of Cardiology also found that “a very favorable benefit-to-risk ratio exists with the COVID-19 vaccine for all age and sex groups evaluated thus far”[20].
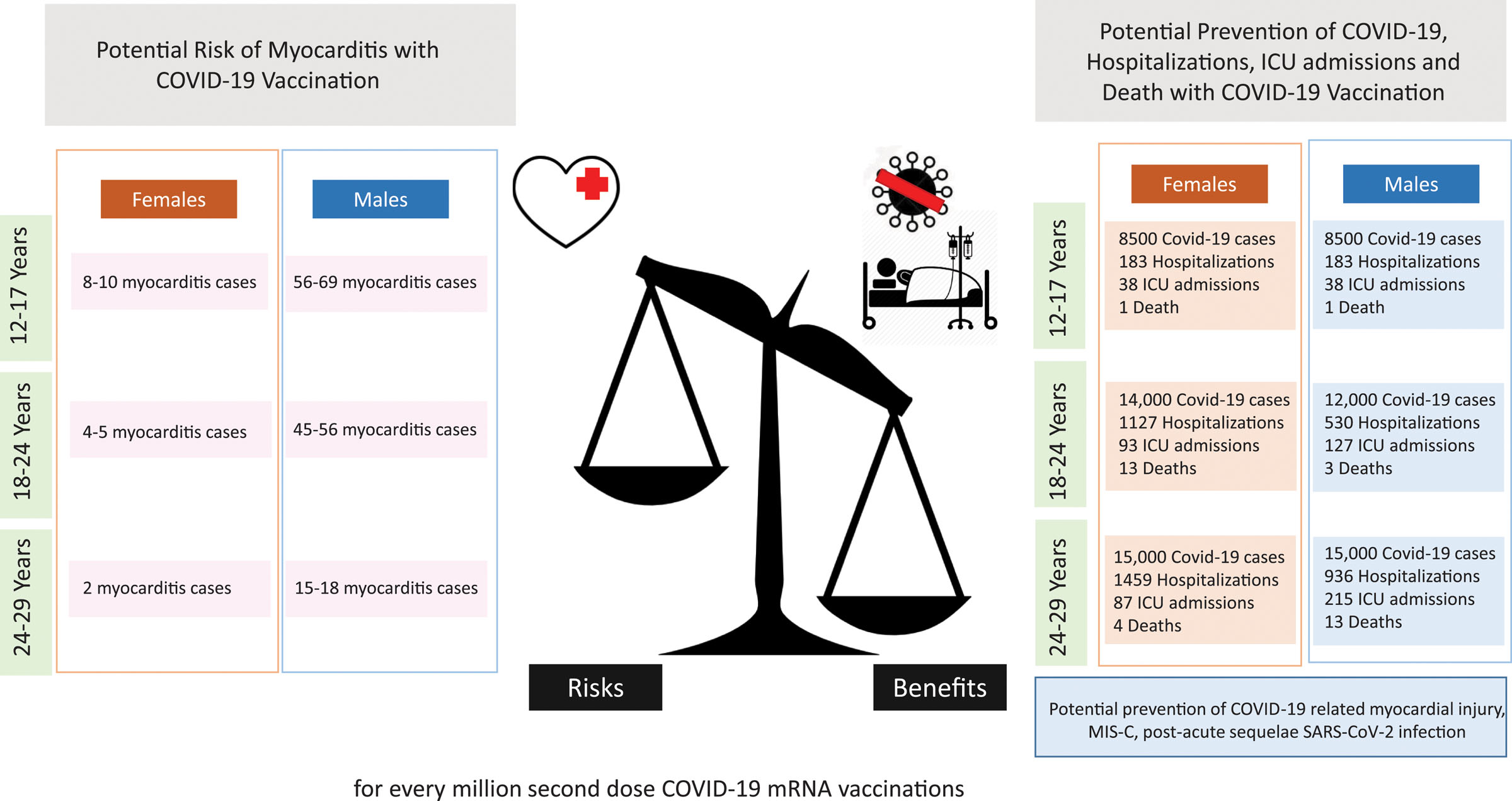
Figure 1 – There is a favorable benefit-to-risk ratio for COVID-19 mRNA vaccine recipients at highest risk for post-vaccination myocarditis[20].
COVID-19 is also associated with a greater risk of developing other health problems, such as blood clotting disorders[21,22] and neurological problems like fatigue and “brain fog”[23-25].
Finally, studies so far haven’t shown that COVID-19 vaccination is associated with a greater risk of all-cause deaths. A CDC study examining the period between December 2020 and July 2021 found a lower non-COVID-19 mortality in vaccinated people compared to unvaccinated people[26]. Another study in more than 520,000 people found that the all-cause mortality was 37% lower in the vaccinated group[27].
On balance, the evidence gathered so far by studies runs counter to the claim made in the Blaze article, showing that the benefits of COVID-19 vaccination outweigh the risks, not the other way around.
Conclusion
The study by Rose et al., used by The Blaze to suggest that myocarditis linked to COVID-19 vaccines carries serious risks, contains important limitations and comes to conclusions that cannot be substantiated by the data it collected. It also grossly misinterpreted at least one study it cited to support its conclusions.
Multiple published studies have shown that the clinical course of COVID-19 vaccine-induced myocarditis is mild for the majority, and contrary to the claims by Rose et al. and The Blaze, don’t entail serious risks of hospitalization and death. Studies have also shown that it is COVID-19—not COVID-19 vaccines—that is associated with a greater risk of cardiovascular diseases and other complications. Reliable scientific studies show that the benefits of COVID-19 vaccination outweigh the risks.
Correction (9 February 2024):
In the Details section, the review initially stated that it is mandatory for healthcare workers to report serious adverse events to VAERS regardless of the cause. It should have specified that this is only the case for the COVID-19 vaccines. We have corrected this error.
REFERENCES
- 1 – Mevorach et al. (2021) Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel. New England Journal of Medicine.
- 2 – Simone et al. (2021) Acute Myocarditis Following COVID-19 mRNA Vaccination in Adults Aged 18 Years or Older. JAMA Internal Medicine.
- 3 – Witberg et al. (2021) Myocarditis after Covid-19 Vaccination in a Large Health Care Organization. New England Journal of Medicine.
- 4 – Montgomery et al. (2021) Myocarditis Following Immunization With mRNA COVID-19 Vaccines in Members of the US Military. JAMA Cardiology.
- 5 – Perez et al. (2022) Myocarditis Following Coronavirus Disease 2019 mRNA Vaccine: A Case Series and Incidence Rate Determination. Clinical Infectious Diseases.
- 6 – Kracalik et al. (2022) Outcomes at least 90 days since onset of myocarditis after mRNA COVID-19 vaccination in adolescents and young adults in the USA: a follow-up surveillance study. The Lancet Child and Adolescent Health.
- 7 – Heymans and Cooper. Myocarditis after COVID-19 mRNA vaccination: clinical observations and potential mechanisms. Nature Reviews Cardiology.
- 8 – Eyre et al. (2022) Effect of Covid-19 Vaccination on Transmission of Alpha and Delta Variants. The New England Journal of Medicine.
- 9 – Prunas et al. (2022) Vaccination with BNT162b2 reduces transmission of SARS-CoV-2 to household contacts in Israel. Science.
- 10 – Singanayagam et al. (2022) Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: a prospective, longitudinal, cohort study. Lancet Infectious Diseases.
- 11 – Jung et al. (2022) Transmission and Infectious SARS-CoV-2 Shedding Kinetics in Vaccinated and Unvaccinated Individuals. JAMA Network Open.
- 12 – Braeye et al. (2023) Vaccine effectiveness against transmission of alpha, delta and omicron SARS-COV-2-infection, Belgian contact tracing, 2021–2022. Vaccine.
- 13 – Maeda et al. (2023) Effect of COVID-19 vaccination on household transmission of SARS-CoV-2 in the Omicron era: The Vaccine Effectiveness, Networking, and Universal Safety (VENUS) study. International Journal of Infectious Diseases.
- 14 – Havers et al. (2022) COVID-19-Associated Hospitalizations Among Vaccinated and Unvaccinated Adults 18 Years or Older in 13 US States, January 2021 to April 2022. JAMA Internal Medicine.
- 15 – Link-Gelles et al. (2023) Estimation of COVID-19 mRNA Vaccine Effectiveness and COVID-19 Illness and Severity by Vaccination Status During Omicron BA.4 and BA.5 Sublineage Periods. JAMA Network Open.
- 16 – Link-Gelles et al. (2023) Estimates of Bivalent mRNA Vaccine Durability in Preventing COVID-19–Associated Hospitalization and Critical Illness Among Adults with and Without Immunocompromising Conditions — VISION Network, September 2022–April 2023. Morbidity and Mortality Weekly Report.
- 17 – Barda et al. (2021) Safety of the BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting. New England Journal of Medicine.
- 18 – Xie et al. (2022) Long-term cardiovascular outcomes of COVID-19. Nature Medicine.
- 19 – Block et al. (2022) Cardiac Complications After SARS-CoV-2 Infection and mRNA COVID-19 Vaccination — PCORnet, United States, January 2021–January 2022. Morbidity and Mortality Weekly Report.
- 20 – Writing Committee. (2022) 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19 in Adults: Myocarditis and Other Myocardial Involvement, Post-Acute Sequelae of SARS-CoV-2 Infection, and Return to Play: A Report of the American College of Cardiology Solution Set Oversight Committee. Journal of the American College of Cardiology.
- 21 – Hippisley-Cox et al. (2021) Risk of thrombocytopenia and thromboembolism after covid-19 vaccination and SARS-CoV-2 positive testing: self-controlled case series study. BMJ.
- 22 – Knight et al. (2022) Association of COVID-19 With Major Arterial and Venous Thrombotic Diseases: A Population-Wide Cohort Study of 48 Million Adults in England and Wales. Circulation.
- 23 – Xu et al. (2022) Long-term neurologic outcomes of COVID-19. Nature Medicine.
- 24 – Wong et al. (2023) Serotonin reduction in post-acute sequelae of viral infection. Cell.
- 25 – Perlis et al. (2022) Prevalence and Correlates of Long COVID Symptoms Among US Adults. JAMA Network Open.
- 26 – Xu et al. (2021) COVID-19 Vaccination and Non–COVID-19 Mortality Risk — Seven Integrated Health Care Organizations, United States, December 14, 2020–July 31, 2021. Morbidity and Mortality Weekly Report.
- 27 – Tu et al. (2023) SARS-CoV-2 Infection, Hospitalization, and Death in Vaccinated and Infected Individuals by Age Groups in Indiana, 2021‒2022. American Journal of Public Health.
