
Fails to grasp significance of observation: The Blaze article wrongly cites a study published in the New England Journal of Medicine as evidence that masks do not work. However, the study did not include a non-mask-wearing group nor was it designed to evaluate the effectiveness of face masks.
FULL CLAIM: “Pro-mask study withdrawn after virus spread in counties analyzed by researchers”; “masks don’t work”; “On November 4, [researchers] were forced to withdraw the study ‘because there are increased rates of SARS- CoV-2 cases in the areas that we originally analyzed in this study.’ Oops. I guess the masks worked until they didn't.”
REVIEW
This article, written by Daniel Horowitz and published by The Blaze on 16 November 2020, claims that “masks don’t work.” To support its claim, it cites the withdrawal of a preprint (a study that has not yet been peer-reviewed or published) uploaded on the MedRxiv server, as well as a published study in the New England Journal of Medicine[1]. The article went viral on Facebook and has received more than 14,000 interactions on the platform, according to social media analytics tool CrowdTangle.
The preprint in question is titled “Decrease in Hospitalizations for COVID-19 after Mask Mandates in 1083 U.S. Counties,” and was authored by researchers at the University of California, San Francisco (UCSF) and Massachusetts Institute of Technology. This preprint was later withdrawn. The article claims that the reason for this is because the researchers “were forced to withdraw the study ‘because there are increased rates of SARS- CoV-2 cases in the areas that we originally analyzed in this study,” and interprets this to mean that masks don’t work.
Health Feedback reached out to the study’s corresponding author, Monica Gandhi, a professor of medicine at UCSF, to assess the accuracy of the article’s claims.
In an email to Health Feedback, Gandhi clarified that, “We were ‘not forced to withdraw this study’. Our study is sound and we have done additional high-level analyses with UCSF big data scientists that clearly show that the institution of mask mandates are associated with reduced severity of disease, even when controlling for incidence (cases). We will be posting the reworked analyses shortly.”
She also added that “There is ample evidence that masks work to reduce transmission, ranging from a series of physical sciences studies to observational studies that show that universal mask wearing reduces transmission[2-5].” [See Gandhi’s full comment below.]
In fact, the notice of withdrawal, which is clearly shown on the MedRxiv preprint, also explains in detail that the reason for the withdrawal was NOT because the data showed that masks don’t work, as the Blaze article claims:
“The authors have withdrawn this manuscript because there are increased rates of SARS- CoV-2 cases in the areas that we originally analyzed in this study. New analyses in the context of the third surge in the United States are therefore needed and will be undertaken directly in conjunction with the creators of the publicly-available databases on cases, hospitalizations, testing rates. Etc. We will be performing this in conjunction with machine learning experts at UCSF. Therefore, the authors do not wish this work to be cited as reference for the project. We hope to have an updated analysis using data from the 2nd and now 3rd wave of SARS-CoV-2 in this country soon. If you have any questions, please contact the corresponding author.”
However, Horowitz predominantly cited the first sentence in the notice, left out most of the authors’ justification for the withdrawal, and then cast the withdrawal in an inaccurate and misleading light.
Next, the Blaze article cites a published study by the New England Journal of Medicine[1], which was conducted on more than 3,000 U.S. Marine Corps recruits, to support its claim. The aim of the study was to determine if the public health strategy implemented by the U.S. Marine Corps for new recruits is effective in reducing the spread of COVID-19. From the study:
“The public health program implemented by the U.S. Marine Corps for all new recruits includes a period of home quarantine followed by a 2-week, strictly supervised quarantine at a closed campus, with the objective of mitigating infection among recruits. To evaluate the effectiveness of these measures, we monitored SARS-CoV-2 infections with serial real-time quantitative polymerase-chain-reaction (qPCR) assays and assessed events of virus transmission by means of phylogenetic analysis of viral genomes obtained from infected participants.”
During the supervised quarantine period, all recruits were required to “wear double-layered cloth masks at all times indoors and outdoors, except when sleeping or eating; practiced social distancing of at least 6 feet; were not allowed to leave campus; did not have access to personal electronics and other items that might contribute to surface transmission; and routinely washed their hands.”
The article claims that “The over 3,000 participants were divided into two study groups, and those who tested positive up front were removed from the group on day 1. By day 14, spread was actually greater among those in the supervised quarantine group (2.8%) than in the control group (1.7%).”
Except that the study did not divide recruits into two groups receiving different treatments, which the claim above suggests. The two main groups in the study were participants (recruits who agreed to take part in the study) and non-participants. Participants were tested at several intervals for COVID-19, whereas non-participants were only tested at the end of the supervised quarantine period. But both participants and non-participants were subjected to the supervised quarantine period and thus both groups had to abide by the same public health measures, including mask-wearing. From the study:
“Otherwise, participants and nonparticipants were not treated differently: they followed the same safety protocols, were assigned to rooms and platoons regardless of participation in the study, and received the same formal instruction.”
This is also indicated clearly in the study’s design, described in its Figure 1 (shown below).
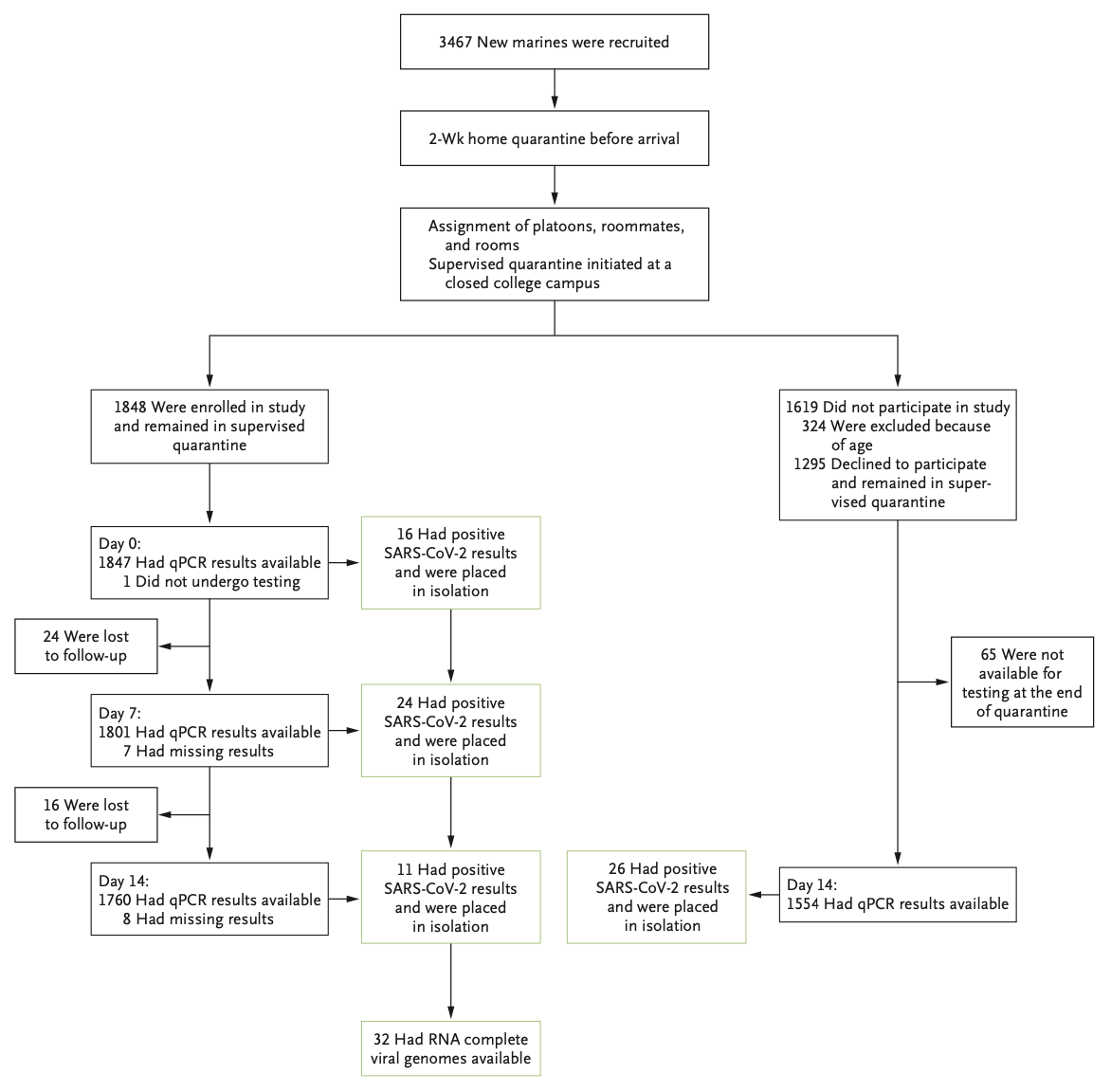
Figure 1. The study design. Of the initial group of 3,467 Marine recruits, 1,848 joined the study and “remained in supervised quarantine,” while of the 1,619 non-participants, 1,295 “remained in supervised quarantine.”
In other words, the study did not include a non-mask-wearing group. It was also not designed to study the effectiveness of masks. Therefore, the comparison made in the article is spurious.
The article claims that “no amount of ‘non-pharmaceutical interventions’ will arrest the spread” of COVID-19. This claim is contradicted by several published scientific studies demonstrating that non-pharmaceutical interventions, such as the wearing of face masks, physical distancing, and lockdowns, can and do reduce the spread of COVID-19, as noted by its effectiveness across multiple geographical regions, including Asia and Europe[6-8].
SCIENTISTS’ FEEDBACK
Monica Gandhi, Professor of Medicine, University of California, San Francisco:
As the corresponding author of this study, I would like to counter that we were “not forced to withdraw this study”. Our study is sound and we have done additional high-level analyses with UCSF big data scientists that clearly show that the institution of mask mandates are associated with reduced severity of disease, even when controlling for incidence (cases). We will be posting the reworked analyses shortly. There is ample evidence that “masks work” to reduce transmission, ranging from a series of physical sciences studies to observational studies that show that universal mask wearing reduces transmission[2-5] (see also here and here). Our hypothesis is that social distancing and masks reduce the severity of disease via reducing the viral inoculum, even if transmission occurs, and our study provides more evidence for this hypothesis. Of note, many places with rising cases across the country only instituted mask mandates recently and cannot be included in our analysis.
REFERENCES
- 1 – Letizia et al. (2020) SARS-CoV-2 Transmission among Marine Recruits during Quarantine. New England Journal of Medicine.
- 2 – Hendrix et al. (2020) Absence of Apparent Transmission of SARS-CoV-2 from Two Stylists After Exposure at a Hair Salon with a Universal Face Covering Policy — Springfield, Missouri, May 2020. Morbidity and Mortality Weekly Report.
- 3 – Wang et al. (2020) Association Between Universal Masking in a Health Care System and SARS-CoV-2 Positivity Among Health Care Workers. JAMA.
- 4 – Lyu and Wehby. (2020) Community Use Of Face Masks And COVID-19: Evidence From A Natural Experiment Of State Mandates In The US. Health Affairs.
- 5 – Gallaway et al. (2020) Trends in COVID-19 Incidence After Implementation of Mitigation Measures — Arizona, January 22–August 7, 2020. Morbidity and Mortality Weekly Report.
- 6 – Cowling et al. (2020) Impact assessment of non-pharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: an observational study. The Lancet Public Health.
- 7 – Hsiang et al. (2020) The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nature.
- 8 – Flaxman et al. (2020) Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature.
